Overview according to cancer stage:
Stage I – II
Radiotherapy is the main choice of treatment. Radiotherapy will cover the nearby lymph nodes even though they are not involved. This is preventive (prophylactic) radiation because some patients may have cancer cells in these lymph nodes that cannot be detected. Selected patients with Stage II NPC may have chemoradiotherapy.
Stage III – IVA
Patients with higher stages of NPC usually receive induction chemotherapy followed by chemoradiotherapy to the nasopharynx and the neck lymph nodes.
Radiotherapy
Radiotherapy is the mainstay of treatment for NPC. External beam radiotherapy uses high energy radiation beams to destroy cancer cells. The delivery of external beam radiotherapy is usually by intensity-modulated radiotherapy (IMRT) or tomotherapy. This treatment allows highly precise radiation beams to be concentrated at the tumor. This could effectively kill tumor cells and, at the same time, reduce radiation damage to the surrounding normal tissues.

Figure: Intensity-modulated radiotherapy for NPC
Procedure:
- Before starting radiotherapy, the patient will have a thorough examination by a dentist to check for dental and oral health. Since radiotherapy can cause tooth decay, damaged teeth may need to be removed before radiotherapy.
- The treatment team will arrange a planning session. The patient will have a mould (shell) of the head and neck that keep the patient very still during each treatment session. The radiation therapist may also make marks on the mould. They will use these marks to line up the radiotherapy machine for each treatment. The patient will then have a planning CT together with the mould.
- The radiotherapy team will then use the information from the CT scan and decide on the radiotherapy plan. Beam information from the planning CT will be sent to the machine for treatment delivery.
- Treatment will be carried out on a daily basis (from Monday to Friday) for six to seven weeks. Each treatment will last for 15 to 20 minutes.
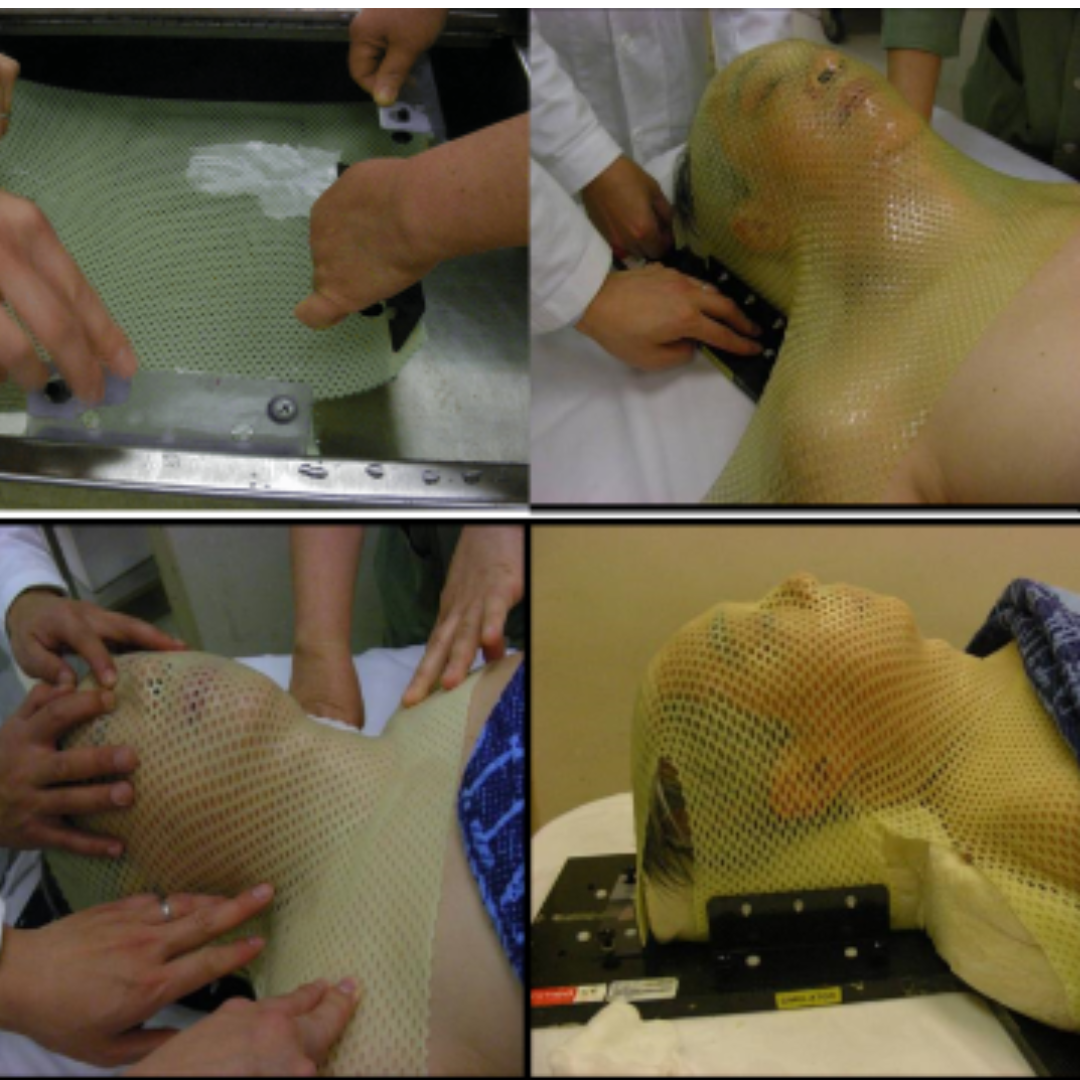
Figure: moulding before planning CT for fixing the body
Side effects:
- Tiredness and weakness
- Redness and irritation of the skin in the treatment area
- Sore mouth and throat
- Difficulty in chewing and swallowing
- Dry mouth
- Change of taste and loss of appetite
- Hearing impairment or loss
- Hypothyroidism
- Swelling in the neck or face (lymphedema)
Chemotherapy
Patients with higher stages will receive chemotherapy. Chemotherapy will be given either together with radiotherapy (chemoradiotherapy) or on its own (before or after chemoradiotherapy).
For chemoradiotherapy, patients will receive chemotherapy and radiotherapy together. Chemotherapy drugs make cancer cells more sensitive to radiotherapy. Chemotherapy is usually given intravenously through a tube placed into a vein. The drugs that are commonly used together with radiotherapy are cisplatin or carboplatin. They are usually given weekly or every 3 weeks.
For patients with Stage III to Stage IVA NPC, chemotherapy may be given before (induction chemotherapy) or after (adjuvant chemotherapy) chemoradiotherapy. The extra chemotherapy aims to control the disease and reduce the risk of recurrence. The chemotherapy may include a single drug or a combination of drugs. Examples include:
- Cisplatin and Gemcitabine
- Cisplatin and 5-fluorouracil (5-FU)
- Cisplatin and Capecitabine
- Cisplatin and Docetaxel +/- 5-FU
- Capecitabine
Side effects:
- Fatigue
- Increased risk of infection
- Nausea and vomiting
- Loss of appetite
- Weight loss
- Sore mouth and dry mouth
- Change of taste
- Diarrhea or constipation
- Bleeding and bruising easily
- Hair loss
How do nasopharyngeal carcinoma patients take care of themselves?
Patients need to be aware of many issues before and after radiotherapy and during recovery. More understanding can help patients face the illness positively.
Regular follow-up and examination
- After radiotherapy, patients may have complications such as otitis externa (inflammation of the external ear), dermatitis (inflammation of the skin) or malfunctioned organs etc. Regular follow-up ensures appropriate treatment.
- Regular follow-up and examination (including fiberoptic nasopharyngoscopy, EBV DNA, MRI, etc) may also allow early detection of recurrence or metastasis, which allows early treatment.
Prevention of decayed teeth and mouth infection
- Radiotherapy will reduce the secretion of the salivary glands, so patients may have higher chances of tooth decay. Therefore, they should:
- Consume less sweet food and drinks, brush their teeth immediately after meals, and visit dentists regularly for checkups.
- Keep the mouth moist: patients may wipe their mouth with clean gauze moistened with salt water before they sleep.
- Stop smoking and drinking alcohol to prevent exacerbation of dry mouth.
Mouth exercises
- Radiotherapy may cause lockjaw. Patients should do mouth exercises every day to enhance the flexibility of their mouths.
Diet
- Patients should consume a high protein and high caloric diet to help speed up recovery.
- Avoid foods that are deep fried, spicy, or dry and hard
- Drink nutritious supplements to increase energy intake.
Skincare
- The skin and lips within the radiotherapy treatment area may be burnt. Patients should:
- Avoid using soap, medicated cleanser and skin lotion. Use mild skin lotion instead
- Avoid direct sunlight and UV light.