Liver cancer was the fifth commonest cancer in Hong Kong and accounted for 4.5% of all new cases in 2023 There were 1,700 new cases of liver cancer in 2023. Over the past ten years (2014-2023), its incidence had reduced by 8.0% from 1,847 in 2014.
The male to female ratio was 3 to 1. The crude annual incidence rate per 100,000 population was 22.6.
Liver cancer was the third leading cause of cancer deaths in Hong Kong. In 2023, a total of 1,408people died from this cancer, accounting for 18.7% of all cancer deaths.
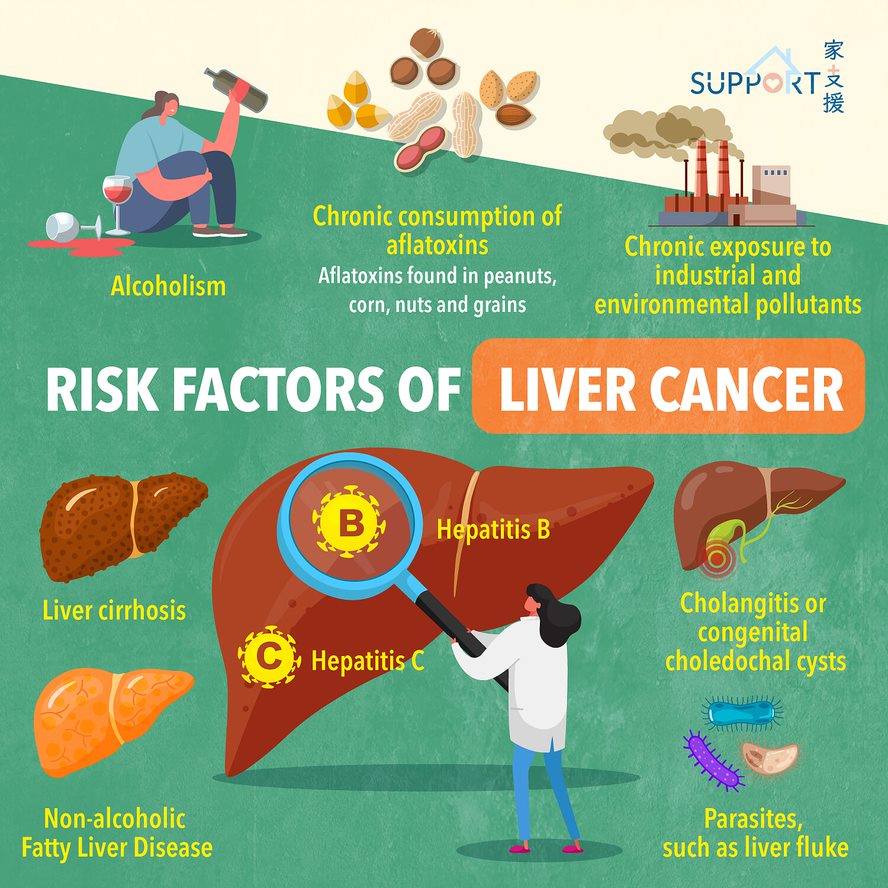
Liver cancer is relatively difficult to cure because the cancer is usually diagnosed in the mid or late stage. Prevention is always better than cure. We should get the hepatitis B vaccination. In addition, hepatitis B virus carriers should also attend regular follow-up to check for signs of cancer development.
What is liver cancer (hepatocellular carcinoma)?
The liver is a very important metabolic organ. It is found on the upper right of the abdomen, comprising the left lobe and the right lobe. The main functions of the liver include:
- Producing and storing glucose for necessary use
- Producing bile for digesting fats in food
- Detoxifying toxins and alcohol
- Producing proteins, blood-clotting components, antibodies and cholesterol
Liver cancer will develop when liver cells begin to mutate and split uncontrolledly. It is further divided into:
- Hepatocellular Carcinoma (HCC), arising from liver cells
- Cholangiocarcinoma or bile duct cancer, arising from the cells lining the bile duct