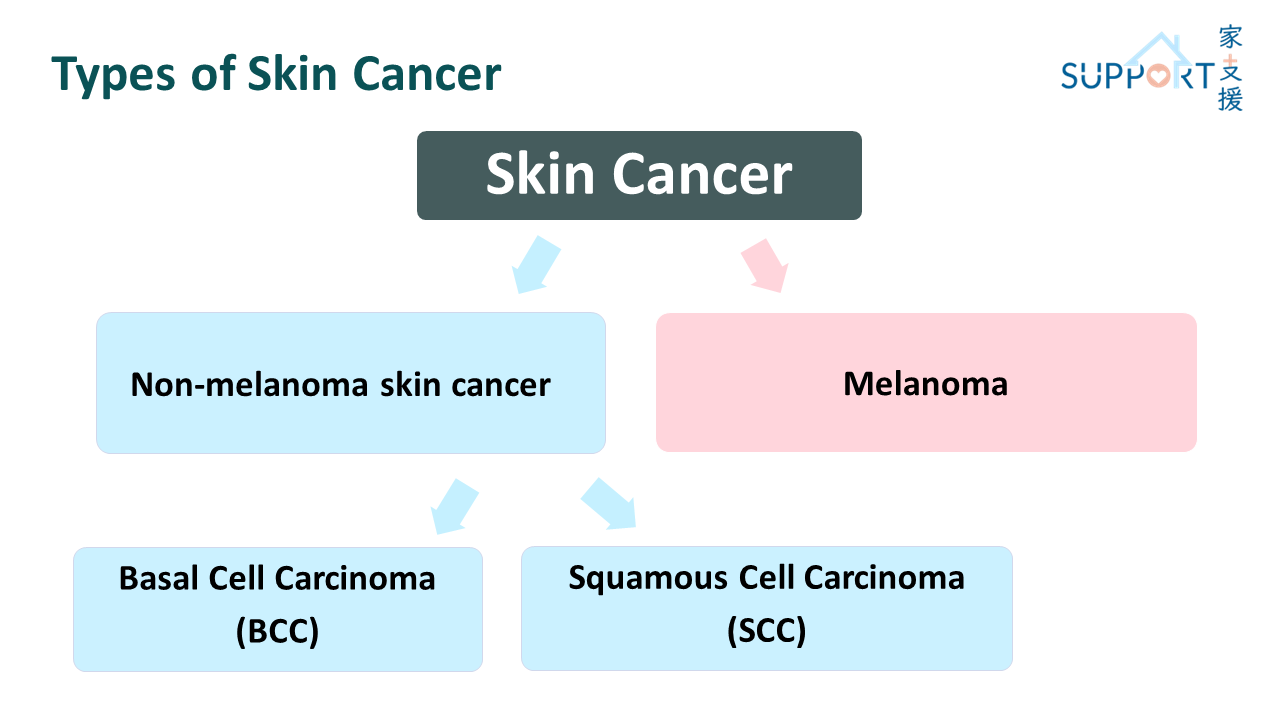
Skin cancer was common in Hong Kong, among which, non-melanoma skin cancer accounts for over 90.7%. Non-melanoma skin cancer ranked the eighth common among males in 2023.
In 2023, there were 1,087 new cases of non-melanoma skin cancer, accounting for 2.9% of all new cancer cases in Hong Kong. The crude annual incidence rate of non-melanoma skin cancer per 100,000 Hong Kong population was 14.4.
The incidence rate of skin cancer in Hong Kong is much lower than that of the Western countries. However, the local number of new non-melanoma skin cancer cases rose significantly by 15.5% from 2014 to 2023.
Although the incidence of skin cancer is high, its mortality rate is relatively low. Since the skin is the most visible organ, most abnormalities can be easily detected. There were total 23 people died from non-melanoma skin cancer in 2023, accounting for 0.2% of all cancer deaths.
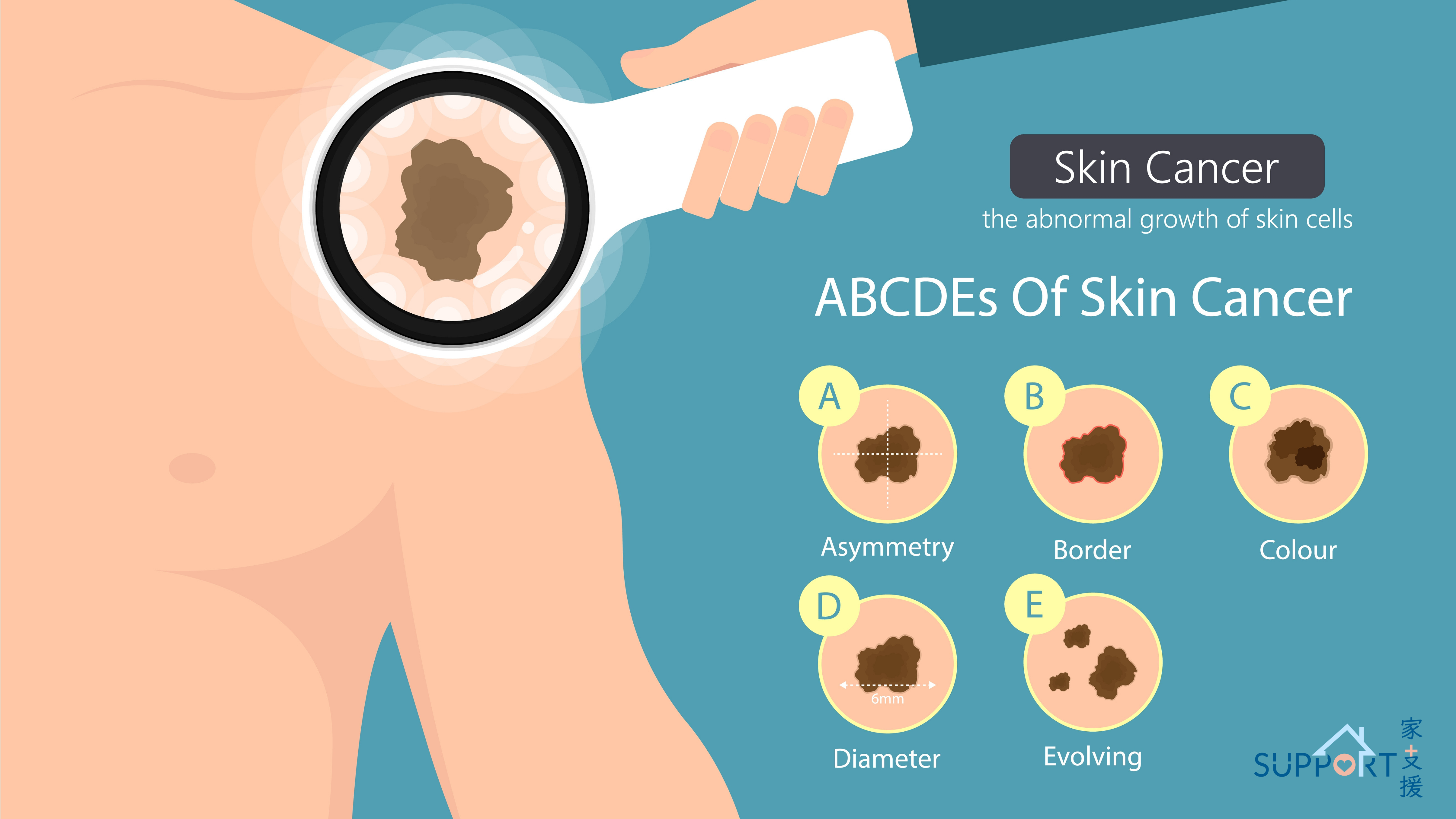
If any unusual skin changes are noticed, please visit a doctor as soon as possible. Early detection increases the chance of successful treatment.
What is skin cancer?
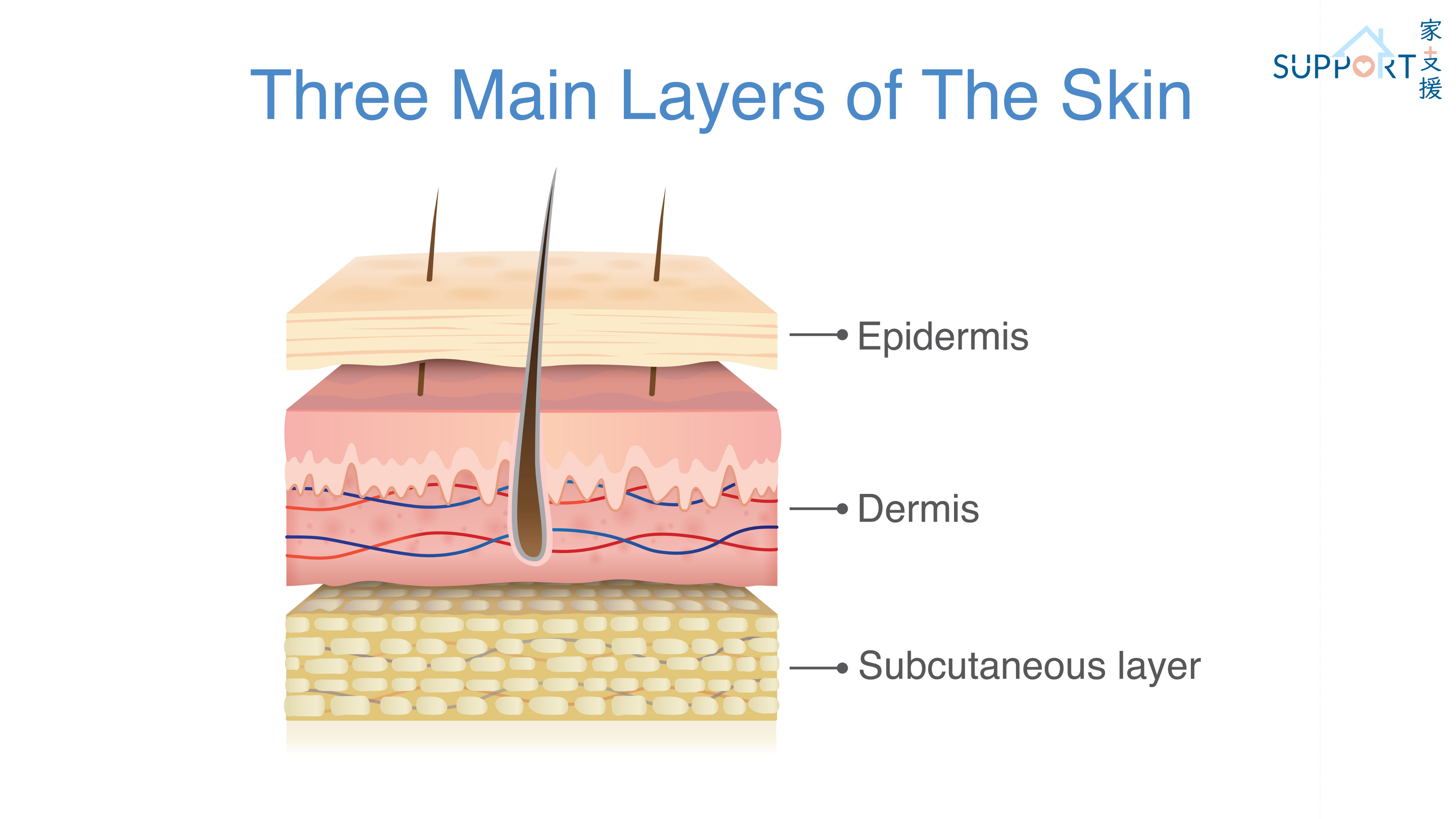
- Structure and functions of the skin
- The skin is the largest organ of the body. It consists of three parts: epidermis, dermis and subcutaneous tissue.
- The epidermis consists of three types of cells: keratinocytes, Langerhans cells, and melanocytes.
- The skin protects the body from foreign agents, lowers the temperature by sweating and prevents dehydration.
- Carcinogenesis
- Skin cancer is mainly caused by ultraviolet rays (UV).
- The main source of ultraviolet rays is sunlight. The second is UV lamps from fitness and beauty centres.
- There are three wavelengths of UV, UVA, UVB and UVC. While UVB is the main mutagenic cause of basal cell carcinoma and squamous cell carcinoma, UVA, which is released in large amounts by tanning beds, mainly causes melanoma.
- UV-related damage to skin is accumulative. Even without sunburn, skin tissues will still be injured after prolonged exposure.
- Previous studies suggested that if skin cells have been damaged at a young age, lack of proper UV protection in adulthood will cause the damaged cells to mutate.
- Skin cancer often appears in areas that are exposed to sunlight, such as the face, lips and neck. However, it can also appear in areas not likely to be exposed to sunlight, such as the palms, soles and gaps between toes.
- Skin cancer which occurs in areas away from sunlight may have genetic factors.